Potential Emergency Department Code Changes Due to COVID-19 Pandemic
By David Bujeda, Senior Architectural Job Captain at BAM Creative, New York
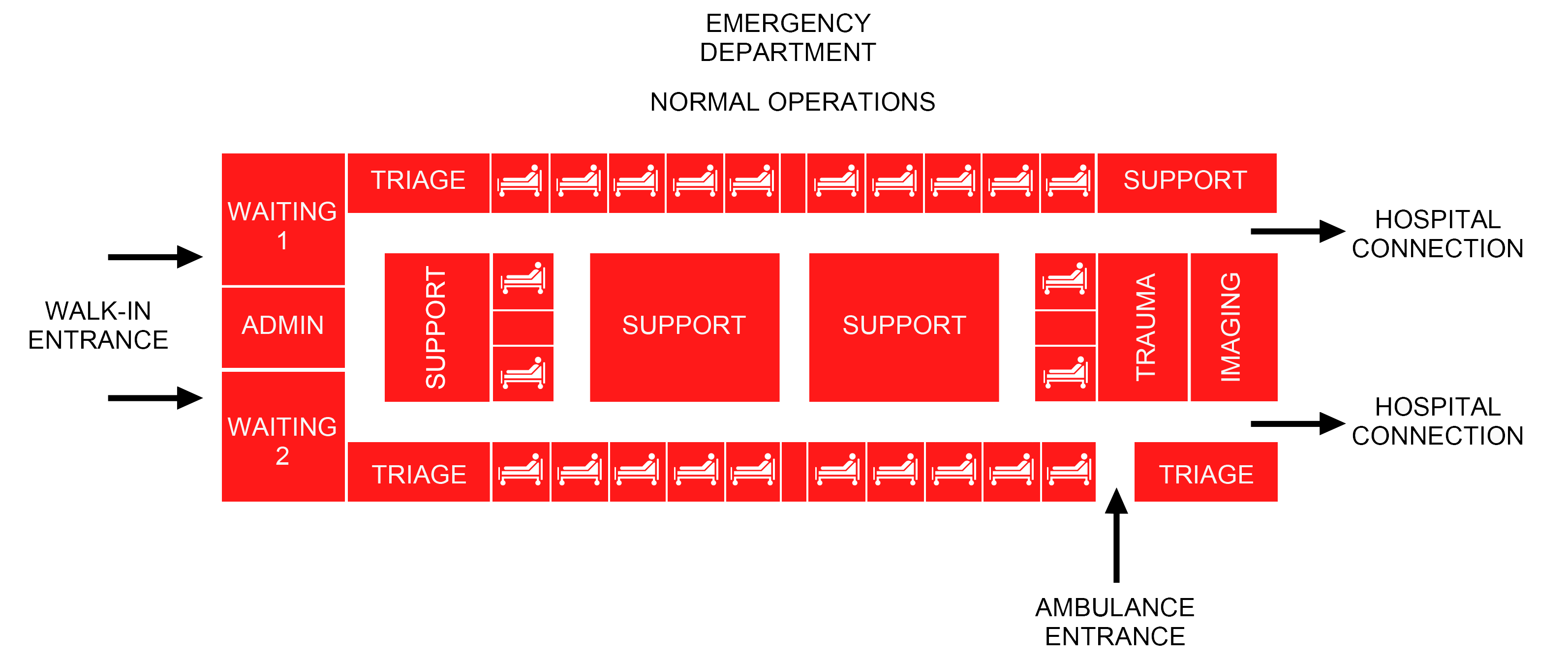
Emergency Departments have been part of the frontline response to the pandemic since the beginning of the virus outbreak. The evolving crisis meant more people confined to home while testing, albeit insufficient, was developed. Any given Emergency Department facility needed to change protocols every day. The evolution of the pandemic during the last year brought up the question of how future Emergency Department needs to be adaptable and responsive to different scenarios, considering that these areas are already the most stressful, versatile, and dynamic in a healthcare facility.
Architects, engineers, and healthcare providers needed to identify strategies to consider the worst-case scenarios. It is vital to rethink flexible spaces and mechanical parameters, with most of the spaces and systems being adaptable to meeting evolving situations and guaranteeing safety of the staff, visitors, and patients.
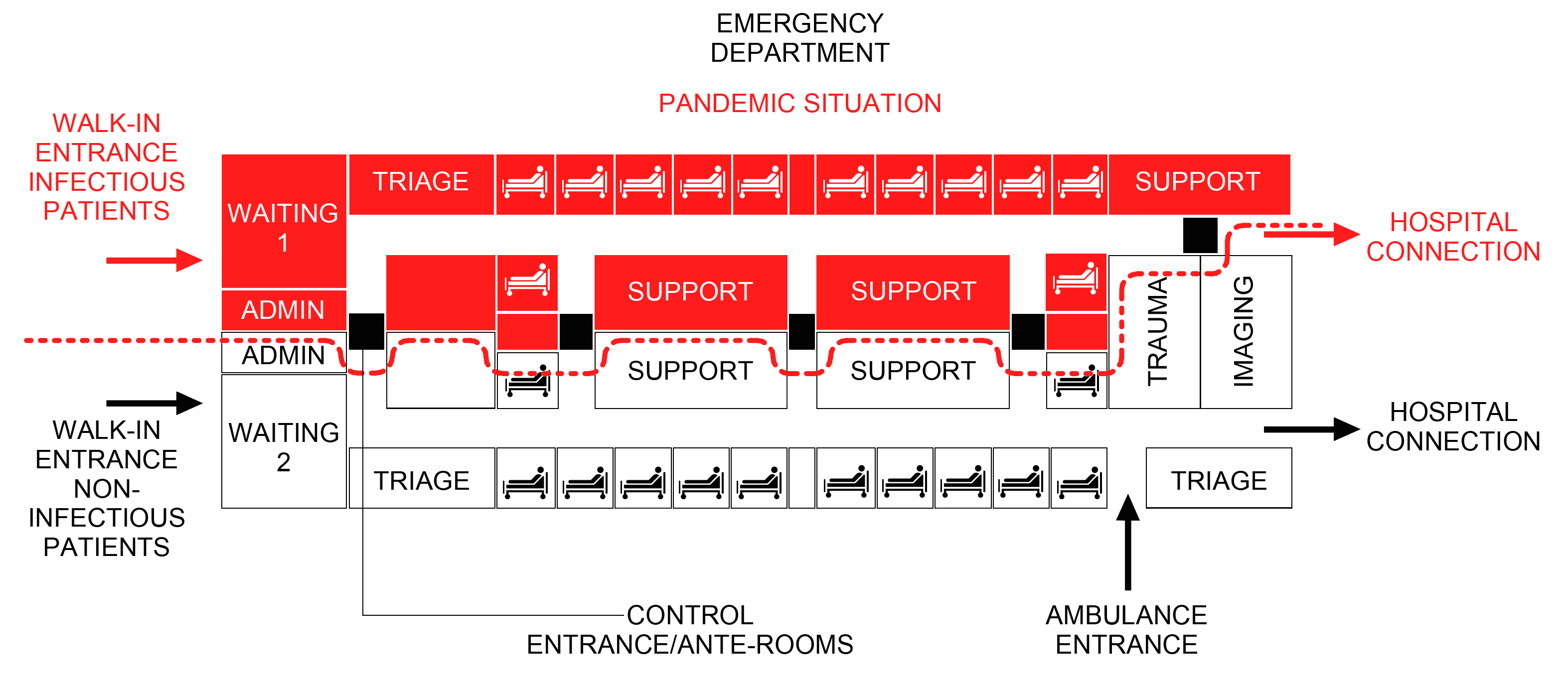
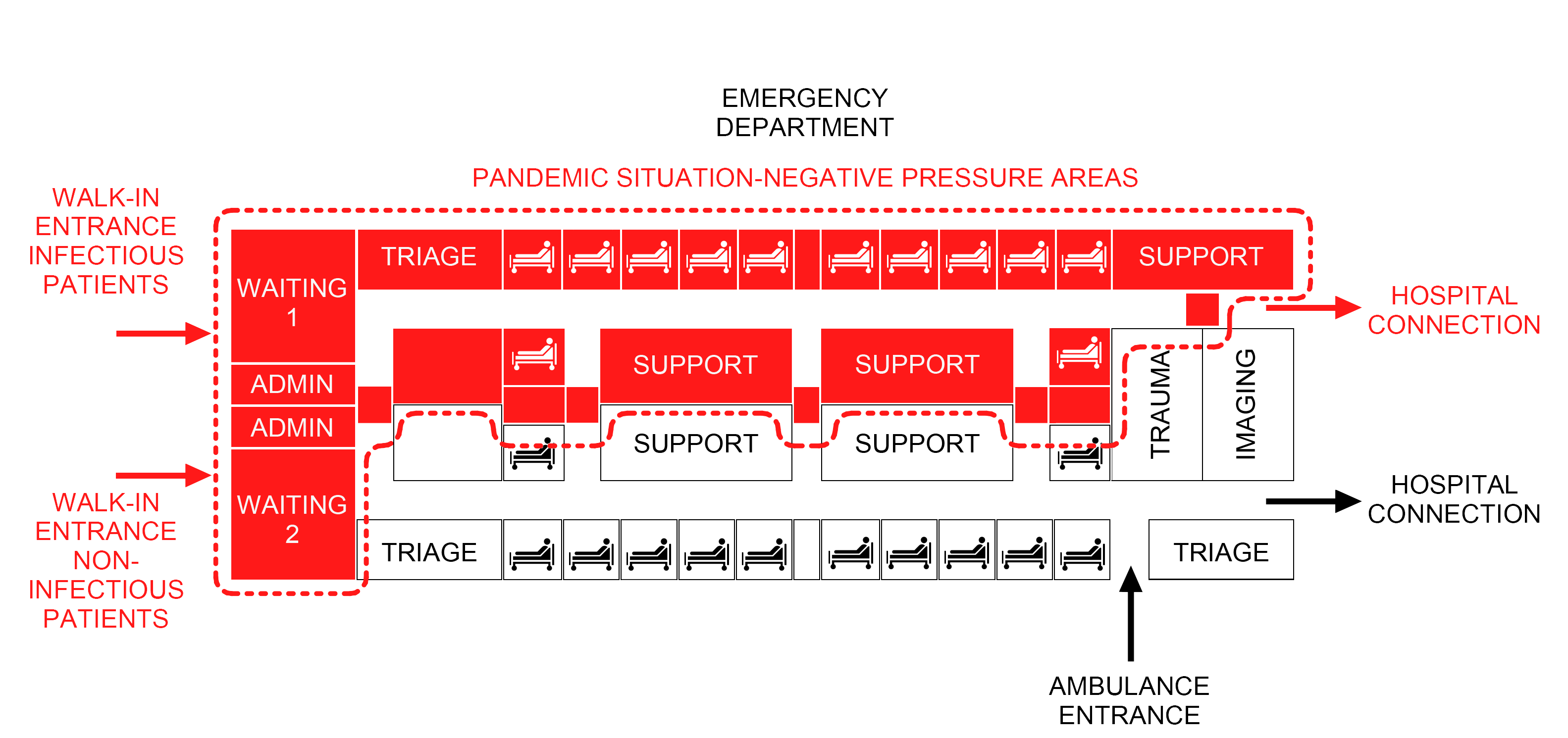
With these premises, we could divide and list the code regulations that need to be reviewed considering these present and future scenarios in three chapters. The first parameters to be redefined would be the safety protocols, which are the initial responses from the hospital staff to react in the event of a pandemic. In conjunction with that, architectural code changes and new requirements would need to be implemented in advance to make the first approach more effective by directing the patients to designated areas in a safe way. The last, and very important with airborne diseases from a mechanical (HVAC) standpoint view: segregating and isolating specific areas to treat infected patients to prevent the transmission to the rest of the facility and maintain a shielded environment.

Summary Diagrams For Emergency Departments